



Blog posts

The biggest misconceptions about agentic AI readiness
To say there’s movement within the agentic life sciences market would be an understatement. According to seven different market research organizations, the “Agentic AI in clinical trials market” is expected to grow at a compound annual growth rate (CAGR) of anywhere between 12.5% and 43%.
While many sponsors and CROs surveyed want agentic AI operating at some level within their clinical trials, almost none of them think they're ready for it. "Our systems don't talk to each other." "Our data is a mess." "We need a two-year foundation project before we can even think about agents." These aren't fringe concerns, they're the default assumptions in nearly every boardroom conversation about AI adoption.
Here's the problem. Those assumptions are very wrong, and they're costing sponsors real time. While teams wait for the "right" conditions to start, the gap between early movers and everyone else keeps widening. The truth is, readiness isn't a prerequisite for agentic AI, it's a byproduct of starting.
Below, we take on the myths that keep organizations stuck in planning mode, and the facts that show why the window to start is now, not after your data is perfectly clean and your stack is fully unified.

What to look for in an AI clinical trial platform: A buyer's guide
Discover what to look for from artificial intelligence tools in the clinical trial market.
Which AI and agentic AI clinical trial vendors integrate best with existing systems?
Artificial intelligence is reshaping clinical trial operations in 2026. Sponsors and CROs are no longer evaluating standalone tools. They are choosing platforms that can connect with existing systems, automate complex workflows, and scale without disrupting ongoing studies. This guide breaks down the vendors best positioned to integrate with the clinical trial infrastructure you already have.

What happened at ASCO 2026
With 44,000+ oncology professionals in attendance, ASCO 2026 may have been the most consequential in recent years. From a standing ovation for pancreatic cancer to the first positive sarcoma trial in history, here's everything that mattered at Chicago's McCormick Place this week.

Real-time clinical trials are here. Medable was built for them.
Real-time clinical trials are here. Medable's continuous trial management platform gives sponsors the evidence generation, agentic AI, and regulatory-ready infrastructure to run clinical programs at the speed the FDA now expects.
Key criteria for evaluating AI and agentic AI clinical trial vendors
Artificial Intelligence is rapidly transforming clinical research. From patient recruitment and protocol design to medical writing and data review, AI-powered solutions are becoming embedded across the clinical development lifecycle. More recently, the emergence of Agentic AI (systems capable of planning, reasoning, and executing multi-step workflows with varying degrees of autonomy) has generated significant excitement throughout the industry.
However, not all AI solutions are created equal. While many vendors promise dramatic improvements in efficiency and productivity, clinical trial organizations operate in one of the most highly regulated environments in the world. Success depends not only on technical performance but also on compliance, validation, governance, security, and trust.
As sponsors, CROs, and technology teams evaluate potential AI partners, they need a framework that extends beyond traditional software procurement criteria. The following considerations can help organizations assess both AI and Agentic AI vendors and identify solutions that are truly ready for clinical research.

The new blueprint for oncology trials: agility, consistency, and scale
Oncology has never been in a better scientific position. Precision medicines, adaptive study designs, and biomarker-driven cohorts have opened up treatment possibilities that simply did not exist ten years ago. But the complexity of running these trials has grown at much the same pace as the science itself, and that gap between scientific ambition and operational capability is where many programmes quietly struggle.
For sponsors building oncology portfolios, and for the CROs executing them, the operational challenge is no longer a peripheral concern. Getting it right comes down to three things: being consistent enough to build efficiently, agile enough to adapt when the science changes, and scalable enough to manage a growing portfolio without the overhead growing at the same rate.
Medable has worked with sponsors and CROs across many global oncology programmes, spanning thousands of sites and participants. That experience has given us a clear picture of what separates programmes that move well from those that get stuck.
Best AI Tools for clinical trial management
Medable is a Palo Alto-based platform that has positioned itself as a leader specifically in decentralized clinical trials (DCT), eCOA, and — most recently — agentic AI. It has been deployed in nearly 400 trials across 70 countries and 120 languages, serving more than one million patients globally, and has been recognized as a Leader in eCOA by Everest Group.

Ontology 101: The semantic layer behind modern life sciences data
Clinical data speaks dozens of languages. Ontologies are the translator. Discover how life sciences teams are using semantic layers, AI agents, and MCP connectors to cut months of data harmonization down to days.
The best AI tools for remote patient monitoring in clinical trials
AI-powered remote patient monitoring (RPM) is transforming clinical trials by enabling continuous data collection, real-time insights, and decentralized participation. This ecosystem spans wearables, AI analytics, data platforms, and decentralized clinical trial (DCT) infrastructure.
Additionally, agentic AI is fundamentally reshaping remote patient monitoring (RPM) in clinical trials by shifting it from passive data collection to proactive, autonomous decision support. Instead of simply aggregating data from wearables and patient-reported outcomes, agentic systems can continuously analyze multi-source trial data, identify emerging risks, and take action, such as prioritizing at-risk patients or sites, triggering alerts, or recommending interventions, without waiting for human input. This significantly reduces delays in detecting safety signals or protocol deviations. Just as importantly, agentic AI introduces workflow automation at scale by handling routine monitoring tasks, coordinating communications, and maintaining audit-ready reasoning trails. The result is a more adaptive and responsive RPM model where clinical teams move from manual oversight to strategic supervision, enabling faster, safer, and more efficient trials.
Below is a structured overview of the leading vendors, tools, and providers enabling AI-driven RPM in clinical research.

The 1:1:1 vision: Reimagining clinical development
"The scarcest resource in clinical trials is the time of the highly qualified people running the clinical trials. We need to free up their time to bring more meaningful innovation to patients."
- David Hyman, Chief Medical Officer, Eli Lilly
Since the year 2000, the pace of drug approvals has remained stubbornly slow, with the FDA approving roughly 50 new treatments per year. This pace is in spite of massive increases in R&D investment. It’s well known that clinical trials take 10-12 years on average to complete all four phases. But what if clinical trials didn’t take weeks to start, months to enroll, and years to complete?

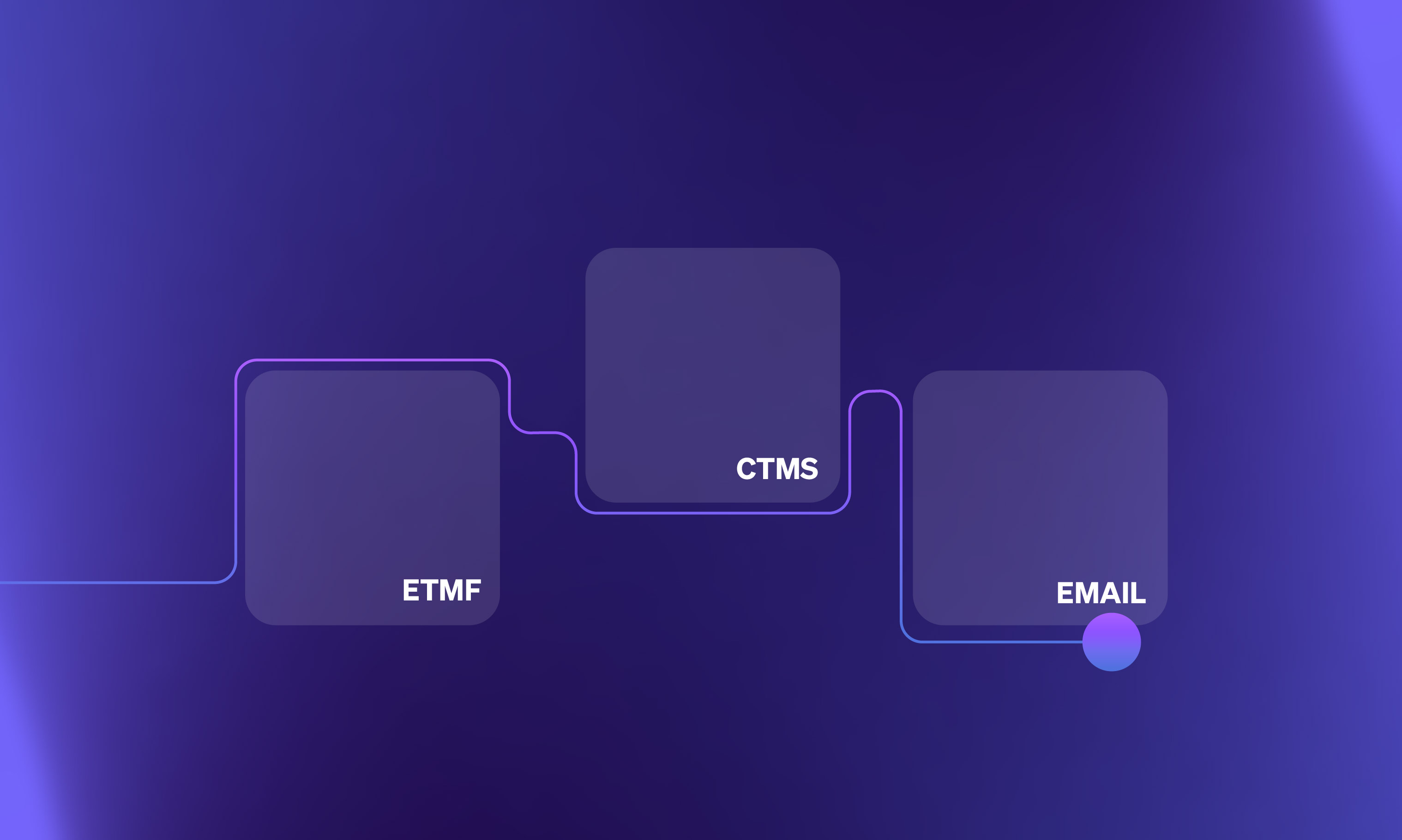
Medable’s Agentic AI connectors and MCPs
Medable’s clinical trial platform leverages a robust network of connectors to integrate seamlessly with the systems that power study execution, from EDC and CTMS to collaboration and data platforms. These connectors enable AI to operate across workflows in real time, unifying data, automating processes, and improving coordination across team

From the Congress floor to the dinner table: A Week in Washington that reminded me why this work matters
There's a particular kind of energy at the World Vaccine Congress that's hard to describe unless you've been in it. Hundreds of scientists, executives, policymakers, pharma leaders, CRO teams, and site networks, all in one convention centre, all sitting with the same fundamental tension. We know how to make vaccines that save lives. So why does getting them to patients still take so long?
I spent three days in Washington this week as part of the Medable team. Washington in late March meant that the cherry blossoms were just past their peak but still stunning, and catching them along the Tidal Basin between sessions was one of those small, unexpected gifts that a busy conference week doesn't always make room for.
For the conference, I came in with a clear intention. I wanted to reconnect with partners I respect, listen more than I talk, and have honest conversations about where this industry is and where it needs to go. What I didn't fully anticipate was how much the week would reinforce something I already believed but needed reminding of.
The urgency is real. And it's shared.